
3 easy steps to identify undercoding
Untap hidden revenue and stop leaving money on the table by reviewing your Evaluation & Management coding.
You may be leaving money on the table by undercoding Evaluation & Management (E&M) services. Give me 10 minutes to help you untap a hidden revenue stream.
Medicare, Medicaid, and commercial payers collect utilization data when processing claims. Each has its own utilization data by specialty, and each payer uses specialty specific data to identify outliers who are overcoding. This data has another use, though, and that is for physicians to assess if they are undercoding relative to their peers. Therein lies an opportunity for you to potentially increase revenues.
Here’s my obligatory disclaimer: I am discussing coding and not documentation. Please make sure your documentation supports your coding levels.
OK. Let’s get to it. Medicare shares its E&M utilization data at the following link: Medicare E&M Code Utilization Tables. The file you need is CY 2016 Evaluation and Management (E&M) Codes by Specialty, which contains its most recent data, found near the bottom of the page. I am going to use Family Practice data from these tables in my example.
Editor's Note: Click here to download a worksheet author Lucien Roberts has prepared to help you identify potential undercoding, described in further detail below.
Step One


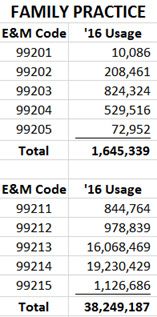
I created a simple spreadsheet, entering the E&M codes for new office patients and established office patients in my first column. I then entered the number of times each was used by Family Practice physicians in my second column.
Family Practice physicians used new patient codes 99201-99205 in billing Medicare 1,645,339 times in 2016. Established patient codes 99211-99215 were used 38,249,187 times. We can see for both that level 3 and level 4 codes are used more frequently.
Step Two


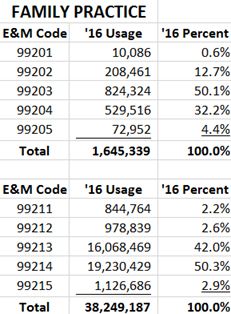
I added a third column to the spreadsheet that converts the count in column two into a percentage. This is calculated by dividing the count for each new patient code by the count of total new patient codes and the count for each established patient code by the count of total established patient codes.
For example, we see that Family Practice physicians used the new patient code 99202 for 12.7 percent of their patients. We can also see 99213 is the code used for 42 percent of established patient visits.
This gives you great baseline data so you can see how often your peers use each E&M code.
Step Three
Fill in the fourth and fifth columns using your own data. Column four will contain counts of the times you used each code. This data should be easy to pull from your practice management system. Column five is the calculation of the percentage of times you use each code. Here’s an example in which I use sample data from mythical Dr. Z.


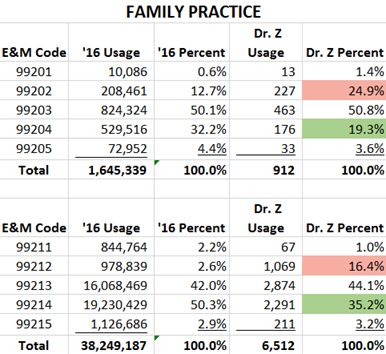
I draw your attention to the highlighted boxes. Dr. Z uses 99202 nearly twice as often as his peers (24.9 percent vs. 12.7 percent). Conversely, he uses 99204 less than two-thirds as often (19.3 percent vs. 32.2 percent). There’s an even greater disparity in his established patient coding, where he uses 99212 more than six times as often as his peers (16.4 percent vs. 2.6 percent) and 99214 far less frequently than his peers (35.2 percent vs. 50.3 percent).
Why does all this matter? Because Dr. Z is leaving a lot of money on the table by coding lower than his peers. For example, Medicare reimbursement for a 99213 is about 66 percent higher than for a 99212.
In other words, you can improve your bottom line starting today if you are undercoding--just make sure your documentation supports your coding. Using the Medicare national fee schedule (Medicare Fee Schedule), I estimate Dr. Z could increase his new patient income by nearly $12,000 (or 11.2 percent) and his established patient income by nearly $56,000 (or 10.3 percent). And because there are no offsetting expenses to this additional income, that money all goes to the bottom line.
In my 25 years of such analyses, I have found that physicians are creatures of habit and code Medicare and non-Medicare services similarly. Thus, the Medicare utilization tables are fairly good proxies for your other payers.
Ten minutes to add 10 percent? It might be one of the best investments of time you make all year.
Lucien W. Roberts, III, MHA, FACMPE, is administrator of Gastrointestinal Specialists, Inc., a 28-provider practice in Central Virginia. He occasionally learns from his mistakes. For the past 25 years, he has worked in and consulted with physician practices in areas such as compliance, physician compensation, negotiations, strategic planning, and billing/collections. He may be reached at muletick@gmail.com.





Asset Protection and Financial Planning
December 6th 2021Asset protection attorney and regular Physicians Practice contributor Ike Devji and Anthony Williams, an investment advisor representative and the founder and president of Mosaic Financial Associates, discuss the impact of COVID-19 on high-earner assets and financial planning, impending tax changes, common asset protection and wealth preservation mistakes high earners make, and more.



