
5 ways to improve patient access
Stanford Health Care learned how to create standardized work to improve patient access and quality outcomes in five areas. These lessons learned can be applied to improve patient outcomes, quality, and service regardless of medical practice size-or budget.
[Editor’s note: This is the first in a two-part series on how to optimize patient access.]
All providers and medical practice leaders strive to provide high-quality care and excellent customer service to their patients. And it’s a major undertaking to accomplish with staff turnover, variable scheduling and rescheduling of patients, diverse workflows, customized physician schedule templates, complex referrals, and numerous other daily activities.
Periodically, it’s important to take pause, think about one’s practice, and evaluate how to improve the multifaceted approaches in meeting patient demand.
Stanford Health Care (SHC) and its medical foundation, University HealthCare Alliance, are working to improve patient access in the San Francisco Bay Area.
We provide more than 1 million patient visits a year in 70 locations with 350 providers in 27 specialties and 1,200 employees. Two-thirds of our providers are primary care while one-third are specialists.
We have worked to interpret the complexities and integration involved in optimizing patient access. It’s no small task for any organization, least of all one that has a diverse group of providers.
Here are five areas where SHC has learned how to create standardized work to improve patient access and quality outcomes. These lessons learned can be applied to improve patient outcomes, quality, and service regardless of medical practice size-or budget.
1. Patient metrics
We realized we needed to pay attention to what we measure. Every practice needs to have a baseline of metrics to measure improvement over time and benchmark oneself against other performers.
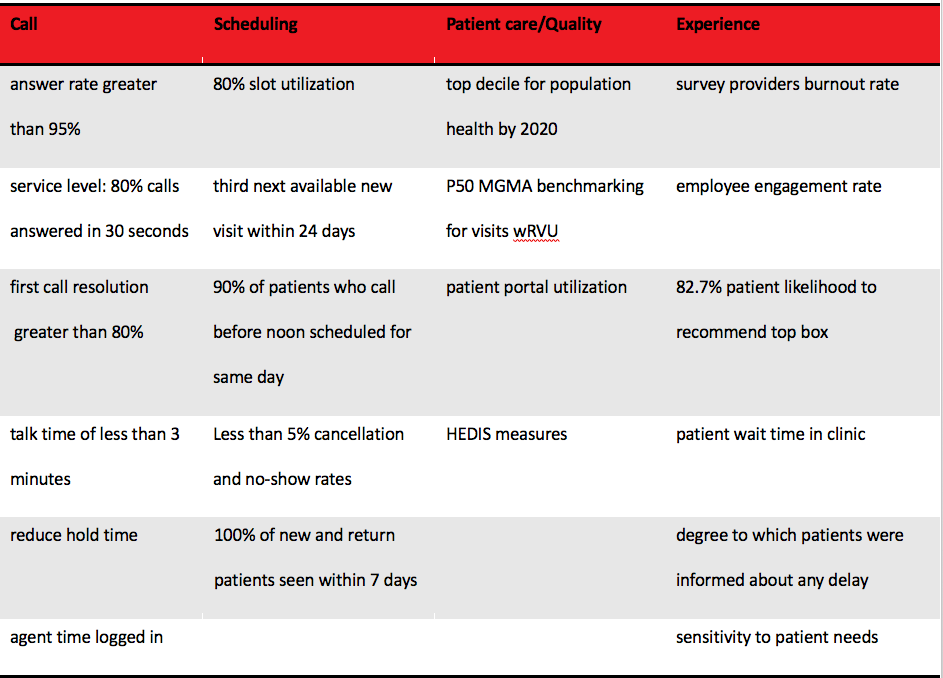
Metrics can be collected manually or abstracted via computer systems. Their value is realized when leaders and staff learn from the metrics and change behavior to achieve expected results.Figure 1 shows several metrics SHC measures to gauge whether our focus on improving patient access continues to be met.
Figure 1:


2. Team-based care
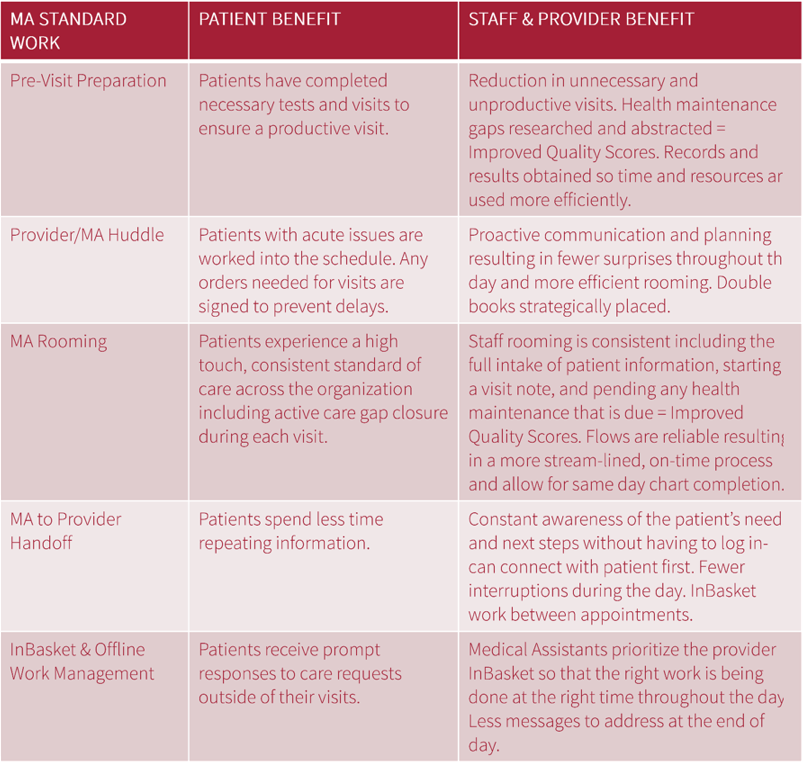
It takes a village. No one person can provide the patient with everything that is needed. Through team-based care, the patient receives coordinated care. A standardized approach ensures a consistent, efficient, and predictable method to deliver care by all members of the healthcare team. More specifically, team-based care creates a strong partnership between the provider and medical assistant to exceed patient expectations (Figure 2). Examples of team-based care include:
- Supplies are provided consistently in each exam room through an organized and clean approach.
- The patient’s first point of contact is meant to have a first call resolution at least 80 percent of the time.
- Appointments are created to allow for new and established patients to get same day access.
- Check-in is hassle free and becomes a personalized experience.
- Visit preparation is done prior to scheduled appointment to ensure that all labs, imaging, results, and paperwork are in place to facilitate an easy visit.
- All visits start on time without delays.
- The patient is connected to the network of care for follow-up referrals.
- Morning and afternoon huddles for providers and medical assistants to review the schedule and anticipate patient needs. During these five-minute huddles, they review details of each appointment; discuss future, standing, or pending orders to be released during the visit; identify double booking opportunities and potential flow busters; and create potential countermeasures.
Figure 2:


The team-based care approach and adherence to standard work will result in many improvements, including better access to providers, staff, and care with more value-added time (e.g., less waiting time, improved cycle time, rapid call resolution, and scheduling response).
3. Call center triage
Patients call the office with questions: She has a rash and wants to know if the provider can prescribe a cream. He has a cough and wants an antibiotic. She ate something that caused her to break out in hives and wants to know what she should do.
Handling telephone calls with these kinds of questions can be a challenge. The goal is to handle them at the first point of contact. But that is not always possible if there are not appropriate clinical protocols and licensed staff who can provide that clinical advice and guidance.
To avoid inefficient call forwarding, message taking, or delays, create a call center that can schedule appointments and answer clinical questions. Otherwise, physicians are bombarded with hundreds of messages that require a response, and it creates delays for anxiously waiting patients.
Having a licensed practical nurse/licensed vocational nurse, registered nurse, physician assistant, or nurse practitioner available to answer clinical questions at the first point of contact creates a better patient experience by effectively and immediately addressing patients’ questions.
4. Scheduling
Patient scheduling can be the bane of a medical group’s existence. If scheduling templates are inconsistent and vary by provider, the opportunity to leverage the electronic health record (EHR) technology is minimized, as there tends to be too many variables to ensure that scheduling is efficient and effective.
Previously at SHC, all providers had their own scheduling guidelines and the ability to block their schedules at will. Provider clinic hours varied based on individual preferences, and there were more than 60 different visit types.
Through a provider engagement retreat, providers and staff made a “Same Day Access Pledge” that resulted in the following changes: standardized guidelines per specialty, fewer than 15 visit types, and access to schedule blocks was restricted to the clinical manager and dyad physician site lead.
Aligning the focus around the patient allowed the providers to open their schedule and allow double booking of patients if necessary to meet patient demand. Through this process, we learned providers were open to seeing each other’s patients. We saw increased patient satisfaction and streamlined scheduling. It was a win-win for everyone.
5. Concierge line
Sometimes, leadership assumes that hospital and health system medical groups must have a centralized scheduling system to create the best patient experience. At SHC, we recognized that creating standardization does not necessarily mean centralization, as demonstrated by the creation of a concierge line.
We drafted a “Rings of Defense” detailing how to best address the patient’s request. In the past, if a patient called a clinic but the schedule was full, the patient had to wait. Under this the new model, if the clinic was full, the staff could provide a warm transfer of the patient to a central location where staff, who had other functions, could work with the patient to secure an appointment at another location.
This process required providers to recognize that if the patient couldn’t be seen today, he/she would go to the emergency room, urgent care, or another provider outside of our medical foundation. Instead, by transferring them to the concierge line, we had staff use the EHR to help the patient be seen by another provider in another location. While the service only handled an average of two patients per day, it gave patients the confidence that we could provide them alternative options to be seen quickly.
This level of creativity and innovation has allowed us to achieve our intended outcomes-improved patient access-without spending a lot of money or resources.
In summary, these five actions allowed SHC to recognize that:
- Tracking metrics consistently lead to successful outcomes.
- A team-based care initiative between providers and medical assistants resulted in a highly efficient patient access program.
- A call center with clinical triaging reduced the number of steps and time needed to schedule an appointment.
- Standardized scheduling guidelines decreased scheduling errors and improved patient satisfaction.
- A concierge line provides staff with an extra level of support to ensure that patients’ needs are met.
Michael O’Connell, MHA, FACMPE, FACHE is senior vice president of operations at Stanford Health Care’s University HealthCare Alliance. Previously, Michael worked as a consultant with The Advisory Board Company in Washington, D.C., and in leadership roles for health systems, hospitals, and medical groups throughout the Midwest. He serves as chair of the Medical Group Management Association’s (MGMA) Certification Commission.









